Corneal refractive surgery is one of the most performed procedures worldwide to correct refractive errors such as myopia, hyperopia and astigmatism. Advances developed in Laser Assisted in Situ Keratomileusis (LASIK) surgery allow greater precision in creating the corneal flap by means of femtosecond laser and lower incidence of complications, among many other advantages. The advent of Small-Incision Lenticule Extraction (SMILE) refractive surgery technique also allows correct refractive errors without altering corneal biomechanics, and is considered a less invasive procedure. However, there are some situations which it is not possible to correct refractive errors through corneal refractive surgery due to high ametropia, irregular cornea, or reduced corneal thickness among others. In such situations when corneal refractive surgery cannot be performed, phakic Intraocular Lenses (IOLs) implantation is an effective alternative that provides excellent visual outcomes, having been reported in multiple scientific researches.
What are the differences between the phakic intraocular lenses?
Phakic intraocular lenses are particularly recommended for the correction of refractive errors in non-presbyopic patients. Currently in addition to allowing correct myopia and hyperopia, toric design of pIOLs also allows correct astigmatism. Different types of phakic IOLs based on their location inside the eyeball have been developed, as angle-supported, iris fixation and sulcus supported phakic intraocular lenses mainly. Logically, the design features of phakic IOLs vary depending on its location, properties and model manufacturer. Precisely the design and location of phakic intraocular lenses is very important to avoid complications such as endothelial cell loss, increased intraocular pressure, lens opacification, pupillary block, among others complications reported in the scientific literature. The incidence of certain complications has determined that some phakic IOLs were withdrawn from the market, and others manufacturers improvements the design to avoid possible complications.

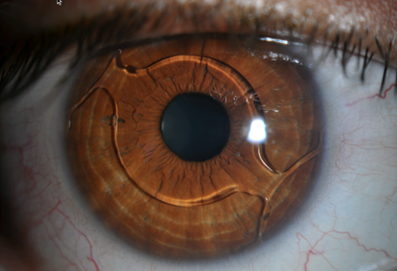
Top image: Artiflex phakic toric intraocular lens implanted vertically. Bottom image: Cachet angle-supported phakic intraocular lens.
In the Online Course “Clinical Methodology in Refractive Cataract and Corneal Surgery” recognized with 25 ECTS credits by University Miguel Hernandez provide extensive training on the clinical applications of phakic IOLs, design features, the calculation of its power and size, the surgical procedure and diagnostic devices that are required to perform. Optical quality of the phakic IOLs, possible complications and the incidence of explant among others will also be analyzed in our program. International tutors of the course are experts in teaching, clinical practice, and scientific investigation about phakic intraocular lenses. Specifically, the professor of the course Dr Reinstein published in the Journal Refractive Surgery an article about the proper size of ICL. In his study conducted in collaboration with others professionals proved that better predictability of postoperative vault height including sulcus diameter into the ICL sizing formula compared with traditional white-to-white-based formula was obtained.
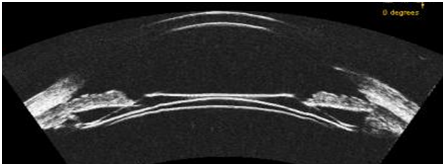
Image obtained with anterior segment Optical Coherence Tomography (OCT) of a posterior chamber phakic lens (epicrystalline).
What other innovations and clinical applications have phakic intraocular lenses?
In addition to being especially useful phakic intraocular lenses for correcting high ametropia or when is not possible to conduct corneal refractive surgery, Artisan iris fixation phakic IOLs allow the reconstruction of the iris, or even pupilar occlusion. Furthermore have been reported in the scientific literature that phakic IOLs are useful in widely clinical applications like patients with corneal ectasies, treatment of anisometropia or amblyopia, correction of high astigmatism after keratoplasty among others. Posterior chamber phakic IOLs have also developed innovations. Precisely, Visian ICL phakic IOL has been developed with fenestration in order to regulate intraocular pressure and avoid possible complications. Multiple scientific researches have developed about phakic IOLs, and we will discuss in the Online Course “Clinical Methodology in Refractive Cataract and Corneal Surgery”.
Bibliographic references
Reinstein DZ, Lovisolo CF, Archer TJ, Gobbe M. Comparison of postoperative vault height predictability using white-to-white or sulcus diameter-based sizing for the visian implantable collamer lens. J Refract Surg. 2013 Jan;29(1):30-5.